Updated July 10, 2025 03:10PM
Solving the Mystery of Swim Deaths
The majority of triathlon deaths happen in the swim. These researchers are trying to find out why—and how to prevent them.

The Norseman 2016 Research Group (Photo: Jorgen Melau)
Dr. Richard Moon took his seat on the airplane, ordered a cup of coffee from the flight attendant, and opened the New York Times. As he thumbed through the Aug. 8, 2011, edition of the newspaper, one headline caught his attention:
Man Dies during New York City Triathlon
A 64-year-old man died after having a heart attack during the swimming leg of Sunday’s New York City Triathlon, race officials said. A 40-year-old woman also had a heart attack during the 1,500-meter swim, according the New York Fire Department. She was in critical condition at St. Luke’s–Roosevelt Hospital Center.
Moon, a professor of anesthesiology and medicine at Duke University Medical Center, knew little about triathlon. But as a medical researcher studying cardiorespiratory function in deep-sea divers, Moon knew more than enough to question why an athletic person, much less one in her 40s, would have a heart attack while swimming. He made a mental note to follow up later, after his flight landed and he had a chance to unpack and catch up on emails. He had all but forgotten this idea the next day, when he opened the New York Times to see a follow-up headline: Second New York City Triathlon Competitor Dies
On a hunch, Moon opened his laptop and emailed the New York City Medical Examiner’s office. His request was an uncommon one, but not completely out of the ordinary for a researcher: Would it be possible to get a copy of the autopsy reports for the two swimmers who died in the New York City Triathlon? It was, and when Moon received the reports, it kicked off an investigation that changed everything we know about swim deaths in triathlon.
ADVERTISEMENT
Although deaths during triathlon races don’t occur often, they do occur—at a rate of about one in every 76,000 participants. Of those deaths, the vast majority—more than 72%—happen in the swim. For years, it was assumed the deaths were simple cardiac events—a heart attack in the water, followed by a drowning. It was a tight and tidy explanation that seemed to fit. After all, the mass swim start of a triathlon is chaotic, full of adrenaline, exertion, murky waters, and 2,000 arms and legs thrashing about—who wouldn’t have a heart attack?
As a result, advice on preventing swim deaths largely centered around risk management. Triathletes were encouraged to visit their doctors and request a full battery of cardiac tests to ensure their bodies were up to the rigors of racing. Risk-reduction efforts included teaching athletes strategies for staying calm in the water, lest the panic of swimming wreak havoc on the heart. Ironman launched a Swim Smart initiative, which encouraged athletes to take a “proper warm-up prior to the start, preferably in the water” in order to increase circulation and decrease the risk of cardiac arrest. Pre-race meetings included a primer on common heart attack warning signs, including pain in the chest, lightheadedness, and jaw pain.
Swim deaths were a dangerous threat, but also one that was generally accepted within the sport. People randomly die from heart attacks all the time—why should triathlon be any exception? When triathletes died in the swim, it was assumed their heart attacks were caused by undiagnosed cardiovascular disease, ill preparation for the intense effort of racing, or simple bad luck.
ADVERTISEMENT
Moon didn’t think it was any of those things. The autopsy reports of the New York City triathletes gave him an indication that his hunch was right. After getting the approval of the Institutional Review Board for Human Research at Duke, he began scanning the news for stories of triathlon deaths. When he found one, he would contact the local medical examiner and request the autopsy report, just as he did with New York City. After collecting about 20 reports, Moon noticed a pattern: triathlon deaths that were often attributed to heart attack were more likely due to immersion pulmonary edema, or IPE. The same thing Moon had been studying in elite Navy divers for years was affecting age-group triathletes.
Dr. Moon begins our interview with an apology:
“I’m so sorry,” he says breathlessly, “I’ve been teaching in the OR, and my computer has been crashing, and it’s just been…” Moon trails off with a sigh. His hair is disheveled and his hospital-issued scrubs are paired with a surgical mask over his ears and under his chin—not because of the operating room, but as a precaution for COVID-19. If anyone enters his office, even briefly, the mask goes up to cover his nose and mouth. The current pandemic is also the reason we are meeting virtually, via videoconferencing, and Moon is slightly flustered by the technology. In part, this is due to the aforementioned computer crashing, but the files and paper piled skyscraper-high in the background also suggest a preference for the old-school way of doing things.
ADVERTISEMENT
That’s not to say Moon is a luddite—a peek into his laboratory will quickly dispel that notion. As Medical Director of Duke University Center for Hyperbaric Medicine, Moon utilizes hundreds of millions of dollars’ worth of advanced medical equipment on a daily basis. The Center studies physiological challenges faced during the exploration of environmental extremes—everything from ocean depths to space exploration. Moon’s team of researchers works to make sense of the symptoms we experience while climbing Mt. Everest, submerged in a submarine, or cycling on Mauna Kea.
Moon has a hand in a number of research projects covering a variety of environments, but his main beat is immersion. His center was funded by the United States Navy beginning in 2007 to investigate a strange phenomenon.
“The Navy, in their SEAL training, has a number of these young, healthy 20-something-year-old trainees who can swim long distances very fast,” explains Moon. “So it was a bit of a mystery as to how such young healthy people could develop pulmonary edema, which is usually a condition associated with heart failure.”
ADVERTISEMENT
Immersion pulmonary edema was first identified in the 1980s by Dr. Peter Wilmshurst, a leading British cardiologist who noticed a string of mysterious drowning deaths of competent divers around the world. It didn’t make sense for experienced divers, who were healthy and well-versed in water safety measures, to suddenly drown. Post-mortem reports cited waterlogged and heavy lungs, consistent with a drowning, yet it didn’t make sense. A breakthrough came when Wilmshurst, himself a diver, encountered a diver in distress during an expedition in England’s Plymouth Sound.
“I was on a boat when two club members surfaced in distress,” Wilmshurst wrote in an early report, “One was dyspnoeic [unable to breathe], cyanosed [blue skin from lack of oxygen], and expectorating bloodstained froth. She said that she had not inhaled water, and that she had had six previous episodes.”
Wilmshurst rushed her to the hospital, where he discovered an accumulation of fluid in the air sacs of the lungs. The condition, known as pulmonary edema, usually occurs as the result of illnesses like pneumonia, exposure to certain toxins, intense exercise at altitude, or trauma to the chest wall. But this diver had none of those things. The more Wilmshurst investigated, the more he uncovered other divers who had experienced pulmonary edema. Some said they didn’t even need to dive to experience their symptoms—simply swimming on the surface of the water caused shortness of breath and bloody sputum.
ADVERTISEMENT
Wilmshurst labeled the condition IPO, or immersion pulmonary oedema; in the United States, the “o” is dropped in “edema,” and condition is referred to as IPE.
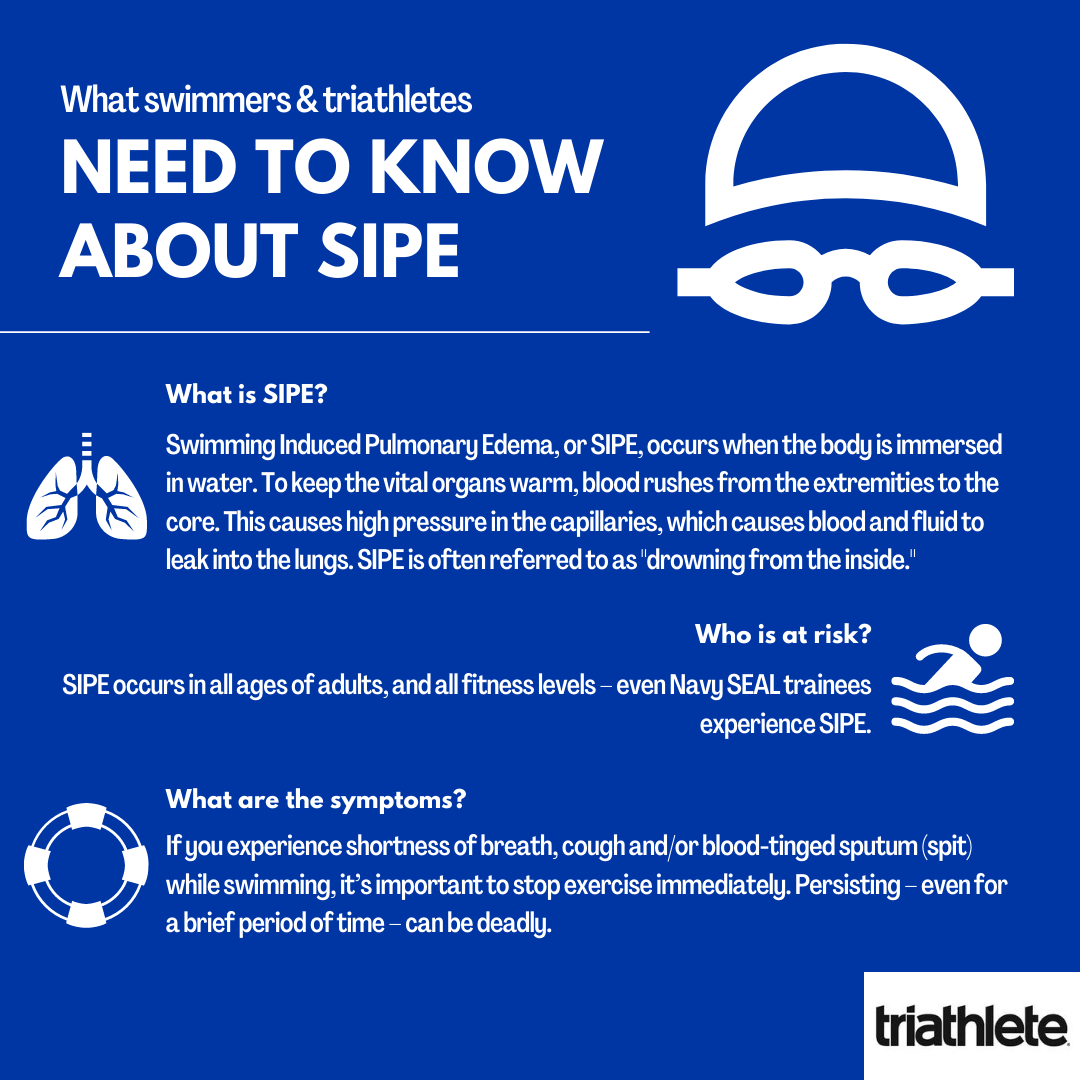
IPE is the rapid buildup of fluid and sometimes blood in the lungs during either swimming or scuba diving, in the absence of ingestion of water. Because water is rarely the same temperature as the human body (98.6 degrees Fahrenheit), the body diverts blood from the extremities and moves it towards the core to stay warm. This can cause high blood pressure in the small capillaries of the lungs, causing a breakdown of the membrane separating the blood from the gas spaces. The result is abnormal leakage of fluid into the alveoli, or air sacs, of the lungs, leading to what is sometimes described as “drowning from the inside.” When IPE occurs, a person experiences coughing, difficulty breathing, blood-tinged sputum, and—in extreme cases—death. When immersion ends and the body warms, the symptoms disappear.
Wilmshurst’s discovery was confirmed when Israeli Special Forces combat swimmers reported the same symptoms in young trainees, followed by competitive and recreational swimmers. IPE became interchangeable with a new name—SIPE, or Swimming-Induced Pulmonary Edema. Moon was called upon by the United States Navy to build on Wilmshurst’s research and help better understand—and, if possible, prevent—SIPE.
ADVERTISEMENT
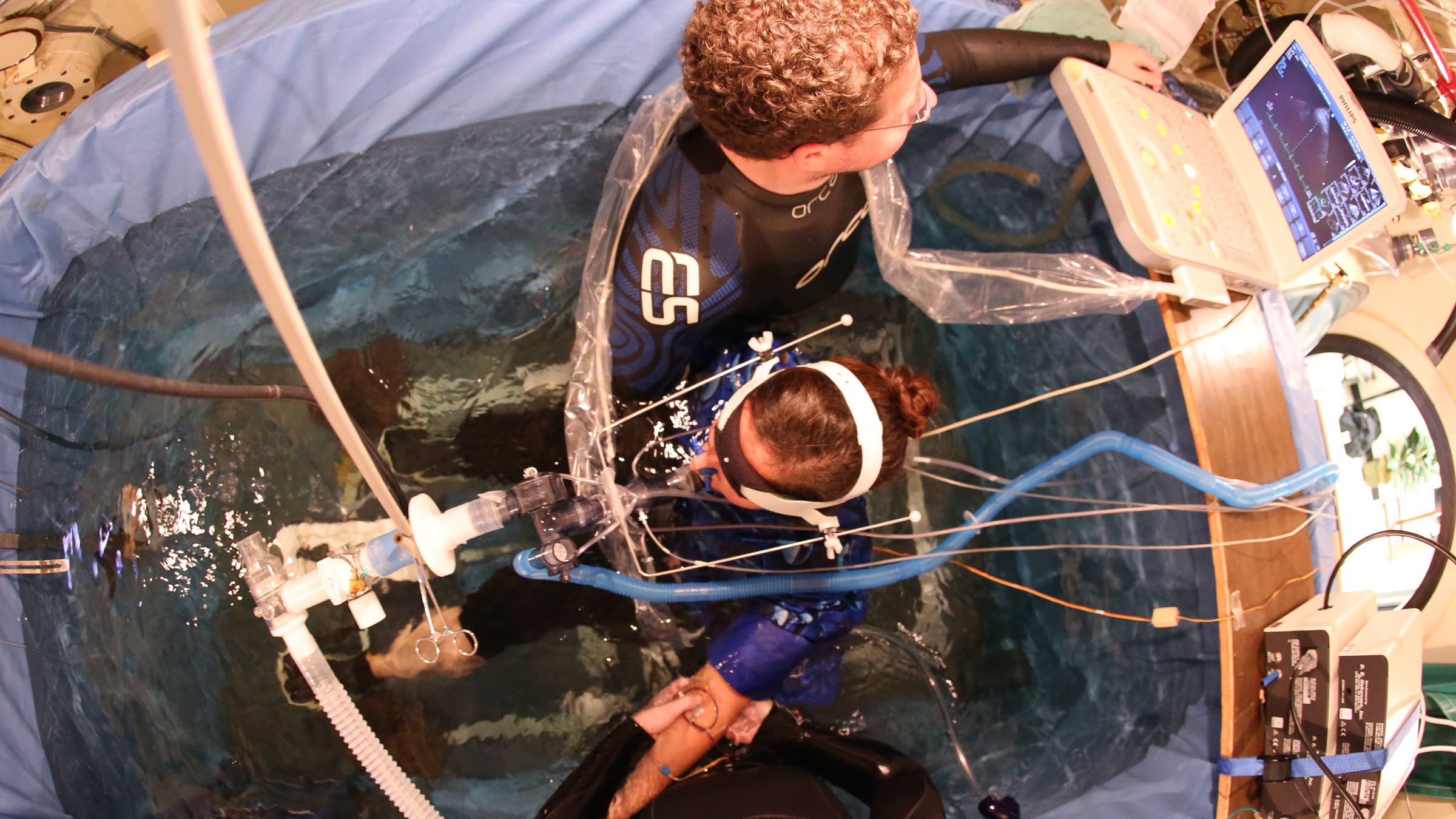
Moon started off with a series of experiments on men and women ranging in age from 20 to 40. Subjects were submerged in 20-degree centigrade water (68 degrees Fahrenheit), then instructed to exercise completely underwater, breathing from an air breathing system.
“Through measurement tools, including an arterial catheter and a pulmonary artery catheter, we could measure actually what was going on in the blood vessels feeding the lung,” explains Moon. “We had a relatively large number who had never experienced immersion pulmonary edema, as normal controls. And then we had those who had experienced SIPE.”
In the latter, a measurement of pressure in the blood vessels in the lung was significantly higher than those who had not experienced SIPE. When the SIPE subjects were removed from the water and treated with a drug to reduce pulmonary artery pressures, their pressures were reduced.
The discovery that immersion pulmonary edema was being caused by high pressures in the vessels led to more questions than answers: “We didn’t know why that was the case, because the people had been screened for heart disease,” says Moon. “They didn’t have heart disease.”
But the location of the pressure—the pulmonary veins (an estimate of the left ventricular pressure after it fills with blood each cycle)—was a blinking arrow pointing to a major clue. As Moon did more research, he found evidence to suggest left ventricular hypertrophy (LVH), a condition that occurs when the muscle in the heart’s main pumping chamber thickens, ultimately may be a factor in many cases of SIPE.
Think of the heart as a balloon. When a full balloon is opened, the air is released passively, while filling that balloon back up takes effort. Thin balloons are easier to fill than thick ones. The same is true of the heart—as it beats, it is filling and releasing, over and over, to move the blood through the body. It requires pressure in order to get the blood in there, and if any part of the heart is thick or stiff, it requires more effort. It’s the same as if you were to blow up a thick balloon—you’ll huff and puff as you blow harder to try to inflate the balloon. In the heart, that pressure cascades down through the pulmonary veins and capillaries.
ADVERTISEMENT
Left ventricular hypertrophy (LVH) is more common in people who have uncontrolled high blood pressure. Left untreated, most people experience no signs or symptoms. But sudden severe blood pressure elevation and heart valve abnormality can—and does—appear in otherwise healthy individuals during extenuating circumstances, like high-stress situations or immersion in cold water, when blood rushes from the extremities to the core. It was those factors—stress and cold water—that served as red flags for Moon when he read about triathlon competitors who died in the swim legs. When he reviewed the autopsy reports, he found that most of the triathletes had LVH, not heart attack. As he gathered more data from more swim deaths, he found most of the athletes whose deaths were originally attributed to simple cardiac arrest had LVH, and only a minority had coronary artery disease. The cause of death in these athletes was more likely SIPE, not a heart attack.
It’s important to note that correlation does not prove causation: LVH is not present in all autopsy reports on swim deaths, and not all people who experience SIPE have LVH. The exact pathophysiology of SIPE still remains elusive. This is partly attributed to its sporadic nature and the difficulty in replicating it under experimental conditions. SIPE may not be one thing, but a combination of simultaneously occurring factors that together create a “perfect storm.” What those factors are, no one really knows yet.
ADVERTISEMENT
This is the insidious nature of researching SIPE: researchers like Moon work for years to find an answer, only to uncover ten more questions. It was once thought SIPE was confined to heavy exertion in cold water; more research has found that isn’t the case. There are cases described during casual snorkeling and leisurely aqua jogging; in cold water, warm tropical waters, and even swimming pools. The original hypothesis of a correlation between duration of immersion and onset has long been disproven, as many cases occur soon after entering the water. One study found tight wetsuits may be a factor, but there are also several documented cases of SIPE where a wetsuit was not worn.
“It’s making a little bit more sense now,” Moon says as he leans back in his desk chair, catching himself just before he knocks over a tower of papers. “But don’t think we’ve completely solved it.”

Understanding swim deaths from the inside out
Somewhere on the shores of Norway’s Eisfjord, Jørgen Melau takes a swig of sports drink. He drops a small silicone capsule—slightly larger than an M&M candy—into his mouth, cocks his head back, and swallows. Then he smiles, adjusts his goggles, and runs into the water.
To most observers on the shore, ingesting a pill before a workout or race may be seen as a curious move—possibly illegal. For Melau, it’s his job. As the safety officer for the Norseman Triathlon in Norway, Melau is simply testing his research tools.
“It’s a combination of familiarizing myself with the research equipment we use and the fact that I like to push myself in training and missions,” Melau says matter-of-factly. “Among other things, I have done hilly intervals in the heat and long swims in cold water connected to my gear.”
ADVERTISEMENT
The “gear,” in this case, is a tiny core temperature body sensor, an ingestible wireless thermometer. Designed to monitor the core temperature of the person who has swallowed it, the pill looks like and is ingested like a regular drug capsule. As it moves through the GI tract, it transmits data to a computer that displays the readings as it records the temperature every 60 seconds during the pill’s journey.
This is one of many high-tech tools Melau and his team use to collect real-time data at the Norseman Triathlon, an event widely regarded as the world’s toughest race. The waters of Eidfjord are cold—some years, as low as 50 degrees Fahrenheit. The shoreline immediately gives way to mountains. The weather is unpredictable, but usually contains at least one element of cold, wet, or windy conditions—sometimes all three. The extreme conditions make it a mecca for physiological research in the field, and each year, dozens of researchers from around the world pack their bags and head to Eidfjord.
There are so many unknowns about SIPE, and we don’t know exactly where to look.
Unlike Moon, who stumbled into triathlon research by accident, many of the Norseman researchers (including Melau) are endurance athletes with a distinct focus on their sport peers. Also unlike Moon, they’re looking at the forest, not the individual trees, in hopes of understanding SIPE.
“There are so many unknowns about SIPE, and we don’t know exactly where to look,” Melau explains. “So we are collecting a considerable amount of data at Norseman—blood sampling, ultrasound of the heart and veins, lung testing, core temperature, and more. In that way, our findings may eventually help in looking for traces on why SIPE occurs.”
Of all the equipment used to study SIPE, Melau says the core temperature pills probably score the highest of what he calls “nerdy gadget points.”
“They are just so cool, that you feel it is something that could be used by James Bond or MacGyver.” Other equipment used in research includes a belt that connects to an electrocardiogram (or EKG) monitor and skin-mounted temperature sensors.
ADVERTISEMENT
Initially, there was some concern about the feasibility of studying athletes in the field using such equipment. It would be understandable for athletes, who have trained for months and years for Norseman, to want to avoid sabotaging their race with unknown variables—what if the pill causes GI distress, or a worn sensor proves cumbersome and annoying over the miles? But Melau says that concern was quickly put to bed when they realized triathletes can’t resist collecting a few nerdy gadget points of their own.
“As it turns out, triathletes are very keen on gadgets in general. So when we ask them, ‘Hey, is anyone interested in swallowing a pill so we can measure the core temperature while you race?,’ there are a large number of hands in the air.”
The data collected during the race provides an important piece of the puzzle, as real-time information may unveil an ingredient (or two, or ten) of the “perfect storm” behind SIPE. Their hope is that collecting and scrutinizing real-time data from the race might uncover patterns in those who experience SIPE. Laboratory studies are insightful, Melau says, but also artificial. “At Norseman, the athletes are pushing their bodies without us as scientists influencing them in any way. The physiology of the athletes is often stretched near to the limits. That kind of intensity is hard to replicate in more controlled studies.”

Perhaps more importantly, having multiple researchers in one place creates a kind of SIPE think tank. Researchers from the public and private sectors, including HUUB wetsuits, the University of Las Vegas, Nottingham Trent University, and Amsterdam University share data and insights in hopes of cracking the code. They voraciously read published studies, like Moon’s, and try to build on the research.
“It’s crucial, because you cannot possibly do everything yourself,” says Melau. “You need input and good ideas from other researchers.”
As a research topic, SIPE can sometimes feel like a moving target—just when something seems to make sense, something else comes along to disprove that notion. SIPE researchers also sometimes face an attitude of incredulity from others—after all, triathlon is a niche sport, and swim deaths are fairly infrequent. Wouldn’t research skills and resources be better put to use with more pressing concerns?
ADVERTISEMENT
But one thing SIPE research has uncovered is that it’s much more common than originally assumed. Though swim deaths are rare, SIPE survivors are not. The current estimate is that 2% of triathletes experience SIPE; some researchers suggest it could be higher. “And it’s not solely triathlon,” Melau adds. “The difficulties around SIPE have been known in the military combat diving communities for years. And then there are swimruns, open water swim races, aquathlon, professional and recreational diving, and more. So this is something we have to consider seriously.”
Symptoms of SIPE
Diagnosing SIPE is about as straightforward as SIPE itself, which is to say: not very. Those who have experienced SIPE often have a similar tale, starting with the onset of symptoms and ending with their hands in the air, as if to say, “I guess we’ll never know.”
The clinical picture of SIPE is a combination of shortness of breath, cough, and/or pink or bloody sputum while a person is immersed in water. Many triathletes try to push through, assuming the shortness of breath is from effort or panic, and the cough from accidentally swallowing water. They don’t always see the color of what they cough up, especially while being in the water.
Because of this, some triathletes chalk up their experience to a panic attack or strange reaction to the water. SIPE never crosses their mind. For some, this is a one-off experience, never to return again; for others, it becomes progressively worse.
“If they end up in the medical tent, or they go to the emergency room, they may discover their oxygen levels are low,” says Moon. “That would be cause for following up.” A chest X-ray would reveal pulmonary edema, but even then doctors may be reluctant to diagnose SIPE. That’s because diagnosing SIPE is really a process of elimination. Could they have had a heart attack? Is there heart valve disease or a cardiomyopathy, where the heart muscle is not contracting normally? Emergency room doctors are trained to look for the obvious conditions first: “When you hear hooves, think horses, not zebras,” is an old chestnut of medicine.
ADVERTISEMENT
If a predisposing factor is found in this process, that’s what gets treated. But what happens if testing happens and nothing is found, as is the case with so many SIPE survivors? Some doctors chalk the experience up to takotsubo cardiomyopathy, a stress-related failure of the heart muscle that develops in a transient way as the result of an intense emotion or physical experience.
“So the brain is experiencing some stress, maybe emotional stress,” Moon explains. “Many people who have it have had things like a recent death in the family or some terrible thing. Or, conceivably it could be caused by racing; you know, they’re all charged up in the water and then everyone’s flailing around them. Of course, stress could be the trigger.”
In these cases, SIPE survivors may return to the water in low-stress ways—a social swim with friends, for example—only to be discouraged by the return of their symptoms. Moon often hears from frustrated athletes who, while searching for answers, discover his research and want his second opinion on the battery of tests they’ve endured. By that point, process of elimination can usually let Moon conclude the issue is SIPE. “What else could it be?” he shrugs.
Although it’s not yet clear exactly how and why SIPE happens, enough is known to test the various hypotheses on prevention. Though many medical conditions require the development of unique therapies and new pharmaceutical treatments, Moon believes a drug for SIPE may already exist.
“Sildenafil,” says Moon. “You may know it by the name brand Viagra.”
Yes, that Viagra—the medication used to treat erectile dysfunction, or the inability to keep an erection. Before it was the “little blue pill that could” (and the subject of eyebrow-raising television commercials), the sildenafil compound was originally developed by Pfizer for the treatment of pulmonary hypertension and chest pain known as angina. During clinical trials, however, researchers discovered the drug was more effective at inducing erections than it was treating angina. Pfizer saw an opportunity to rise to prominence for creating the first oral treatment for erectile dysfunction, and with it, major financial gain. In its first quarter, Viagra brought a total of $400 million in revenue for Pfizer, and would later produce annual sales of about $1.8 billion.
ADVERTISEMENT
The pop-culture phenomenon of Viagra eclipsed prescriptions for its originally-intended purposes—specifically, treating hypertension. In both sexual and cardiac applications, sildenafil works by relaxing the muscles in the walls of the arteries, allowing the blood vessels to become wider. This reduces the pressure in the arteries and allows blood to flow more easily through them. This relaxation happens throughout the body, which is why it works to increase blood flow in both the heart and to the penis.
Of course, the idea of giving sildenafil to triathletes before a swim leads to a lot of immature chuckles. Spandex tri suits and tight wetsuits, after all, are probably the last thing anyone wants to wear with an erection. But Moon says any sexual effects are dependent upon sexual arousal and stimulation—Viagra itself does not spontaneously cause an erection. Many people take the drug for pulmonary hypertension without embarrassing results. More importantly (at least in the study of SIPE), people take the drug without impact on their athletic performance. That, coupled with what Moon calls a “chain of evidence,” presents a compelling case for a clinical trial.
“So we have a plausible rationale why sildenafil may work—that’s number one,” says Moon. “Second, we have a physiological study showing that it should work, based on the pressures we observe when studying SIPE. Where we’re at now is a clinical trial.”
ADVERTISEMENT
In his current study, Moon puts subjects who have experienced SIPE through two experiments: in one, the subject receives a sildenafil pill an hour before exercise, the other a placebo pill. During the exercise portion of the study, subjects ride a stationary bike for 40 minutes while immersed in cold water. Researchers track physiological data as well as any symptoms of SIPE which appear (if and when SIPE occurs, the exercise is stopped immediately and the subject removed from the water). The protocol is repeated at least one week later, with the pill swapped, for comparison.
If successful, Moon’s hypothesis will be confirmed: A prophylactic dose of sildenafil, taken before the swim start, can reduce the risk of SIPE. Such a discovery won’t eliminate swim deaths completely, but it could reduce the number significantly. For SIPE survivors who have quit swimming out of an abundance of caution, sildenafil could provide an opportunity to return to the sport safely.
The major challenge of the study is recruitment. Despite offering a stipend, finding men and women with a SIPE diagnosis who are also willing to travel to the Duke University campus in North Carolina presents major logistical challenges. The COVID-19 pandemic has also put human research studies on hold, but Moon hopes to resume soon. “The original plan was to be finished with a study by September of this year. You know, that may not happen because of coronavirus delays. But if I could get another 12 people in the study by December, I’d be ecstatic.”
Preventing deaths in the triathlon swim
Until answers are found, SIPE deaths will occur during the swim of triathlon races—unless, of course, there’s a way to spot them before they happen.
ADVERTISEMENT
Some researchers, such as those at Norseman, are already tracking physiological data in hopes of spotting patterns that would make it possible to catch SIPE in real time. Others have robust educational programs for athletes and volunteers, akin to what was used for heart-attack education of yore (only this time, they’re getting the information right with SIPE signs). At Ironman Mont-Tremblant, they brought out the drones.
The idea of using drones as a swim safety and rescue tool during a swim race came by way of Dr. François de Champlain, an emergency physician and trauma team leader at McGill University Health Centre in Montreal. After several years of successfully serving as the medical director of the Rock ‘n’ Roll Montreal Marathon and ITU Montreal Triathlon, de Champlain was tapped to take the helm of medical services at Ironman Mont-Tremblant 2018. Though he was excited for the new challenge, the race was massive compared to what he had done before.
ADVERTISEMENT
“I was used to doing medical direction for Olympic-distance triathlons and marathons. You have 42K [26.2 miles] to cover with your medical team there. You don’t have legs of 180 kilometers [112 miles] of cycling or a four-kilometer [2.4-mile] swim to cover with your medical team,” says de Champlain. “That’s a massive playground, and you can never have enough medical staff to have a quick response.”
De Champlain was tasked with finding new and efficient ways to aid athletes in need of medical attention. Ironman officials were particularly concerned about preventing swim deaths. In recent years, the race series had rolled out safety measures within its Swim Smart program, including switching mass starts for smaller waves and rolling starts. It also placed anchored “resting rafts” for distressed swimmers along the course. But what about those who couldn’t make it to the rafts in time? De Champlain knew there had to be a better way to spot and rescue swimmers in distress.
ADVERTISEMENT
Around the time he was appointed to his role with Ironman Mont-Tremblant, de Champlain traveled to Renfrew, Ontario, for a meeting. A team of paramedics had teased some new technology relevant to de Champlain’s charity venture, an organization which uses drones to deliver Automated External Defibrillator (AED) devices to cardiac arrest patients in rural areas where the arrival times for an ambulance are longer.
“So there was a demonstration of their drones, and they presented us with a bunch of footage. I remember vividly this one video he showed us of a collision where they were quite remote from the station, and drones arrived there sooner than the ambulance. The drones could access the site from the air. It had a very cool HD video feed where they could actually assess what was needed on the scene.” Immediately, de Champlain thought of the race. “Wouldn’t it be great help for a medical director to have a helicopter-type view of the situation and say ‘Okay, we need two teams there immediately’ and then you can distribute your resources accordingly.”
ADVERTISEMENT
De Champlain saw a million possibilities for drones at Ironman Mont-Tremblant, but there was one glaring problem: The race was only eight weeks out. “Those guys are very organized, and usually they plan deployments like this for six months in advance. But I’m an emergency physician, so I said we had plenty of time,” de Champlain laughs. After a bit of convincing, the Renfrew paramedic crew was on board for the race, and soon, de Champlain’s colleague and research partner at McGill, Dr. Valerie Homier, was, too. The team developed a research protocol that would, for the first time, test the feasibility of using drones as a swim rescue tool.
De Champlain began by identifying swimmers at risk, using the medical questionnaire all athletes are required to complete. Swimmers with preexisting conditions, such as seizure disorders, cardiac arrythmias, or SIPE, were recruited for the study and given a bright yellow swim cap to help drone operators spot them in a field of competitors wearing race-issued pink and green swim caps.
On race morning, 25 yellow-capped swimmers took to the water, each one followed by a drone. For each drone, there were three team members: a professional pilot operating the drone, an assistant checking the airspace for safety and maneuverability, and a “screen observer” trained to spot signs of distress in swimmers.
ADVERTISEMENT
Though none of the yellow-capped swimmers needed to be rescued from the water that day, five other competitors did. One of those swimmers was spotted by the drone team, who was able to alert lifeguards on the water in time for a rescue. The spotting was a fluke, according to de Champlain, but one that gave him a lot of optimism. “The drone was locked in on one swimmer in the study, but the bigger picture identified another swimmer in the periphery who needed rescue. We thought it was interesting, even though it was not the purpose of the study, there were two purposes of this study, which was really to see if drones could spot a swimmer in distress ahead of the traditional lifeguards on boards, or teams on boats from a water level, where you don’t have an overview of the situation.”
The protocol wasn’t perfect. Some drone teams identified swimmers in distress, only to discover flailing arms were really just people waving—they thought the drones were for media purposes, and were ready for their close-up. There’s also the fallibility of technology: batteries die, propellers break, and winds blow. During de Champlain’s study, intense fog delayed the launch of the drones. There’s also a matter of safety—flying large drones over large crowds of people can be a risky venture. Still, the technology proved it has a place in preventing swim deaths.
“It’s a great tool. You’re going to see this happening more and more,” says de Champlain. “Technology in general is happening more and more.”
ADVERTISEMENT
How robots might save us
Almost every researcher studying swim deaths agrees technology will play a major role in the future. The more we learn about SIPE and swim deaths, the more fine-tuned the technology becomes. Artificial intelligence may one day scan drone footage for signs of swimmer distress, spotting subtle signals humans miss. Other drones could swoop in and deliver flotation devices or even supplemental oxygen. Pills like those used at Norseman may become standard issue for tracking real-time physiological data, or perhaps it might be wearable technology, like a stick-on sensor applied to the skin. When abnormalities appear in the tracking, a light might blink or a vibration buzz: Please report to the medical tent.
If it sounds far-fetched, it’s not. Technology is already used for similar healthcare purposes. Insulin pumps track blood sugar levels and deliver a customized dose to maintain stability. Pacemakers can wirelessly transmit data to a doctor. Smartphone apps and fitness watches are constantly developing new real-time biometric trackers, including blood pressure monitors and sweat sensors to measure electrolyte balance. Wearables have alerted their users to the first sign of illness, sometimes to great surprise.
ADVERTISEMENT
Technology doesn’t get muddled with emotion, and in healthcare applications, that’s an important feature. A person may feel fine (or “just a little tired”), and ignore signs that something is not fine after all. Their oxygen saturation levels or heart rate, measured by wearables, may show a pending medical crisis. Triathletes, who are stubborn by nature, may need such objective analysis of technology. Pushing through the pain may be acceptable for muscle cramps, but with conditions like SIPE, such a decision could be deadly.
“I think those wearables sometimes will give us ideas way before there is a dramatic event,” says de Champlain. “Then there is a way then to communicate with a medical team and say, you know, ‘Could you stop number 123 when she arrives at the mile 16 aid station and check a few things with them before you let her go? Because we had an alarm on one of the biometrics parameters for this participant.’ I think this is the future. It’s going to happen. When it will happen, I don’t know. But I think it’s going to happen sooner than later.”
ADVERTISEMENT
What also might happen soon: A full understanding of SIPE. Though the current picture of SIPE is opaque, each new discovery brings a little more clarity. “We gather as much information as we can and present it in scientific papers. Researchers around the world do the same,” says Melau. “In that way, we get a series of reports that give us a clue on where to look. I believe we are very close to some understanding of how to progress now.”